Papillary Renal Cell Carcinoma: Clinicopathologic Study of 144 Cases with Emphasis on Subtyping
Ahmed Alomari1, Harriet Kluger2, Kenneth Haines1, Dinesh Singh3, Adebowale J. Adeniran1
Departments of 1Pathology, 2Medical Oncology, and 3Urology, Yale School of Medicine, New Haven, CT, USA
ABSTRACT
Background: Papillary renal cell carcinoma (PRCC), a morphologically and genetically distinct subtype of RCC, is morphologically separated into two subtypes for therapeutic and prognostic purposes. In spite of multiple studies, many clinicopathologic issues about PRCC remain vague because the cohorts were small. Our study was designed to review and analyze the clinicopathologic features associated with Type 1 versus Type 2 PRCC.
Design: Our pathology archives were searched for all nephrectomies and kidney tumor biopsies performed between 1985 and 2011, with the final pathologic diagnosis of PRCC. Slides and pathology reports were reviewed. The diagnosis of PRCC was confirmed in each case and subtypes were determined based on established morphologic criteria. Follow-up data was obtained from the clinical database.
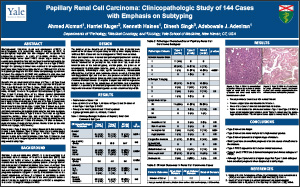
Results: We identified a total of 144 cases (74 Type 1, 46 Type 2 and 24 mixed) – 29 female and 115 male. Mean age was 56.0 years for Type 1 and 59.0 years for Type 2 (range, 23-88 years). Mean tumor size: 3.6 cm Type 1 and 4.6 cm Type 2 (p=0.1). Race distribution: 88 white, 45 black, 11 others. Ten patients had metastases (2 Type 1, 6 Type 2 and 2 mixed). None of the tumors showed sarcomatoid differentiation. Desmoplasia was present in 9% of cases while microscopic scar was identified in 45% of cases. Type 1 tumors were more likely to have nuclear grade 2 and less while Type 2 tumors were more likely to have nuclear grade 3 and above (p<0.001). Type 1 tumors mostly presented at stage 1 while Type 2 tumors were more likely to present at higher stages (p=0.05). Perinephric fat invasion (p=0.004), microvascular angiolymphatic invasion and main renal vein invasion were more likely in Type 2 tumors. There was no significant association between tumor type and renal sinus fat invasion or invasion of muscular branches of renal vein. Follow up information was available in 134 patients: 11 alive with disease, 117 alive no disease, 1 dead of disease, 5 dead of other causes. Median follow up time was 58.5 months (range, 1-272 months).
Conclusions: Type 2 tumors are larger. Sarcomatoid differentiation is a rarity in both subtypes. Type 2 tumors have higher nuclear grades and present at higher stages than type 1 tumors. Type 1 PRCC appears to have better clinical outcomes than Type 2. Based on long follow-up data, both subtypes appear to have excellent prognosis when diagnosed at early stage.
©2013 Yale Department of Pathology. All rights reserved.
Any redistribution or reproduction of part or all of the contents in any form is prohibited. You may not, except with express written permission of the author or the Department of Pathology, distribute or commercially exploit the content, nor may you transmit it or store it in any other website or other form of electronic retrieval system, including use for educational purposes.