Cytopathologic and Molecular Diagnostic Clues to Poorly Differentiated Thyroid Carcinoma: A 10-year Single Institution Experience
Liying Fu MD, PhD1, Xiangbai Chen MD, PhD1, Berrin Ustun MD1, Julie Ann Sosa MD2, Sanziana Roman MD2, Elizabeth Holt MD3, Manju Prasad MD1, Adebowale J. Adeniran MD1, David Chhieng MD, MBA1, Renu Virk MD1, Constantine Theoharis MD
Departments of 1Pathology, 2Surgery, and 3Internal Medicine, Yale School of Medicine, New Haven, CT, USA
ABSTRACT
Background: Poorly differentiated thyroid carcinoma (PDTC) is a rare thyroid neoplasm with clinical behavior between differentiated thyroid carcinoma and anaplastic thyroid carcinoma. PDTC often displays insular architecture, necrosis and increased mitotic activity on histopathologic evaluation. However, there are few studies describing cytological features of this rare tumor, which are important for a preoperative diagnosis. In this retrospective study, we review our experience in the fine needle aspiration (FNA) diagnosis of PDTC.
Design: Cases of PDTC were collected from our archives, a tertiary referral hospital, between the years 2002-2012. Of 21 cases surgically diagnosed as PDTC, 16 patients had preoperative FNA evaluation and were included in this study. Four cases had BRAF mutation analysis in addition to cytological evaluation. These cases were retrospectively reviewed by two cytopathologists.
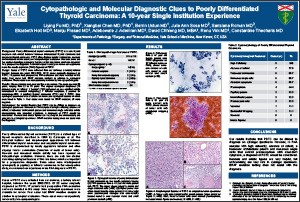
Results: Eleven patients were men and five were women. The mean age was 56 years, ranging from 22 to 70 years. The original cytological diagnoses (16 patients) were as follows: 1 “benign” (FNA performed on one calcified nodule contralateral to eventual malignancy), 7 follicular neoplasm, 2 positive for malignancy-NOS, 4 papillary thyroid carcinoma (PTC) and 2 PDTC. Nine cytological specimens were available for review, the cytological features of which were listed in Table 1. Four cases were tested for BRAF mutation; all were negative.
Conclusions: Our results illustrate that PDTC can be difficult to diagnose on cytological specimens. However, in FNA samples with high cellularity, absence of colloid, a trabecular architectural pattern and numerous single cells that exhibit pleomorphism with abundant cytoplasm, a diagnosis of PDTC should be considered. Necrosis and mitotic figures are very helpful, but unfortunately, are very rare in cytological specimens. BRAF mutation testing does not assist with the diagnosis.
©2013 Yale Department of Pathology. All rights reserved.
Any redistribution or reproduction of part or all of the contents in any form is prohibited. You may not, except with express written permission of the author or the Department of Pathology, distribute or commercially exploit the content, nor may you transmit it or store it in any other website or other form of electronic retrieval system, including use for educational purposes.