This patient has intestinal metaplasia (Barrett esophagus). Grossly note the presence of islands or extensions of ("salmon pink") mucosa rising into where squamous mucosa ("pearly white") should be. In Barrett esophagus, the squamous epithelium is replaced by intestinal-like columnar cells in response to the reflux of gastric acid into the esophagus. This adaptation substitutes mucinous epithelium which is more resistant to damage by gastric enzymes than squamous epithelium.
Barrett metaplasia often has well-formed goblet cells that can be visualized using a mucin stain.
Intestinal metaplasia is reversible (with elimination of the reflux). It is associated with a higher risk of cancer, typically adenocarcinomas arising in this area and is therefore considered a pre-malignant phenomenon. It is not, however, dysplastic. Metaplasia results from the reprogramming of stem cells which give rise to all mature epithelia (squamous, gastric, or intestinal).
Other examples of metaplasia include the change from ciliated respiratory mucosa in the bronchi to squamous epithelium in response to tobacco smoke. "Smokers cough" results from this loss of ciliated epithelium (the mucociliary escalator).
Next, you examine the patient's esophagus and stomach.

Compare the gross and microscopic finding of the gastroesophageal junction of your patient to a normal.
What type of epithelium do you expect in the esophagus? the stomach?
Does the glandular epithelium in your patient remind you of normal epithelium from another location?
What type of change is this?
Can you think of other examples of this change?
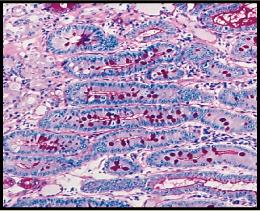
This image is a "special stain" (i.e. not H&E). What type of stain could it be and what is is staining?
Which of the following statements about this condition are true?
It is reversible.
It is associated with a higher risk of cancer.
It is a type of dysplasia.
It is a pre-malignant phenomena.
It is a disorder of stem cells.
It causes gastroesophageal reflux.

