Red infarcts occur tissues with dual circulations (e.g. the lung and small intestine) where the unobstructed parallel arteries pump blood into the necrotic zone. Lung, in particular, because of its spongy nature can collect lots of blood in the infarcted area. Venous occlusions (or even severe stasis) can cause red infarcts. In addition, if an arterial occlusion is removed (e.g. thrombolysis), the restored blood flow can burst through necrotic (ischemic) vessels.
Because of the dual circulation in the lung, larger vessel obstructions can lead to hemorrhage without infarction.
White infarcts occur when an artery in a solid organ (with end-arterial circulation) is blocked. Such organs include the kidney, spleen, and heart.
Infarcts tend to be "wedge" shaped (as with the examples here) because obstruction of a proximal vessel results in downstream infarction of the distal branches that radiate away
Pulmonary emboli (PE) frequently arise in the deep veins of the leg (deep venous thrombosis or DVT) and travel through the right heart into the pulmonary artery. Patients that are immobilized (post-surgery, airplane travelers, patients with casts) are at particular risk. In cases where a large PE enters the pulmonary artery, it can straddle the pulmonary artery bifurcation (a "saddle" embolus). In such cases death is immediate because of obstruction of the pulmonary circulation. However, even small PEs can cause fatal cardiac arrhythmias.
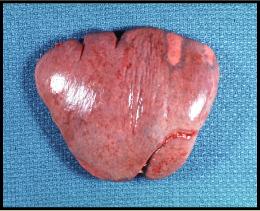
The bottom images of the spleen show a white infarct. In this case, the thrombus would have developed somewhere between the left atrium and the splenic artery. Had it developed in the venous circulation it would have become a PE (unless the patient had a septal defect in the heart or a patent ductus arteriosis). Most arterial infarcts are due to thrombus formation over an area of vessel damaged by atherosclerosis. Alternatively the left atrial appendage (particularly in cases of atrial fibrillation) or aneurysmal dilation of the left ventricle can provide a pouch where large thrombi can develop.
Other type of emboli include septic emboli (discussed in a later lab), amniotic fluid emboli, air emboli, and fat and bone marrow emboli).
Embolic injury is also an important cause of infarction. Below are two images of infarcts due to embolisms.
What organ are affected?
Infarcts are referred to as "white" or "red" depending upon the organ affected. Why do infarcts appear different in different organs, and what organs are more likely to have red vs. white infarcts?

This is a case of embolization of a thrombus.
Where might the thrombus have developed?
What conditions predispose patients to this type of embolus?
Frequently in this organ, emboli do not cause
infarcts. Why?

This image shows a large embolus that has traveled to this organ.
Where is it located? Where did it come from?
In this case, death is immediate. Why?
This is also a case of embolization of a thrombus.
Where might the offending thrombus have developed in this case?
What other types of embolization can you name?

