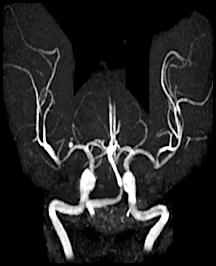



Cerebral hemorrhages are caused by the rupture of a weakened cerebral artery. Several things can undermine cerebral arteries including hypertension (classically occurring in the basal ganglia), atherosclerotic plaque, or aneurysms (such as the saccular or "berry" aneurysm visible in the angiogram to the left). Berry aneurysms usually occur near the circle of Willis. The resulting hemorrhage can occur either within the cerebral parenchyma or the subarachnoid space and can result in cerebral compression from a "mass action" effect.
Thrombotic infarctions are frequently due to the occlusion of arteries by atherosclerotic debris and subsequent obstruction by thrombotic material. Usually these lead to nonhemorrhagic infarctions resulting in liquefactive necrosis.
Embolic infarcts occur when an embolus travels to a cerebral vessel and disrupts blood flow. Classically, embolic infarcts lead to a hemorrhagic infarction, possibly because the embolus dislodges, exposing necrotic brain to the full force of arterial pressure.
Here are 3 angiograms. Each case represents either a thrombotic, hypoperfusion, and hemorrhagic stroke. Which is which?
To help you answer this question. Think about the following.
What would thrombosis of an artery look like on an angiogram?
What is a precursor lesion that can lead to cerebral hemorrhage and what might it look like?
In the absence of hemorrhage or thromboembolic event, would you expect to see any abnormality on the angiogram (assuming the patient recovered)?
 For a hint. Move your mouse over the lightbulb.
For a hint. Move your mouse over the lightbulb.


