




The primary treatment for nonhemorrhagic strokes is the administration of thrombolytics (e.g. tissue plasminogen activator, t-PA) prior to the development of ischemic necrosis. Since thrombolytics would exacerbate hemorrhagic bleeds, the distinction between hemorrhagic and nonhemorrhagic strokes is critical. Fortunately, as you can see, the distinction is quite apparent on a non-contrast CT scan.
Infarcts due to hypoperfusion are generally located in the watershed areas between the major branches of the cerebral arteries. They occur in cases of prolonged ischemia. In such "low flow" states the areas at the farthest end of the circulatory system become hypoxic and, if the hypoxia is prolonged, undergo infarction. Heart failure, sepsis, and acute blood loss are common causes of watershed injuries to the brain.
The large intestine is another organ that is prone to watershed injuries between the branches of the mesenteric arteries (and the sigmoid artery). These are located at the splenic flexure (Griffith's point), the rectosigmoid (Sudeck's point), and the ileocecal region. See the resources page for an extra folio on colonic watershed injuries.
A complication of old cerebral infarcts is that they can rebleed as is the case here. The edema associated with large infarcts can compress local small blood vessels. As the edema subsides, reperfusion of the damaged vessels can lead to hemorrhage.
Non-contrast CT is a critical component for the evaluation and subsequent treatment of strokes.
Why?
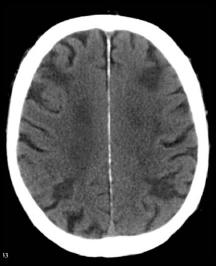
When examining these CTs, remember that collections of blood will be radiodense. Initially infarcted brain will show minimal changes on a CT, but after a few days, there is marked effacement of the normal architecture.
Can you distinguish between these CTs and assign them each to one of the aforementioned categories?
 Where would you expect hypoperfusion injury to occur? Click the question mark for a hint What other organ in the body is prone to hypoperfusion injury?
Where would you expect hypoperfusion injury to occur? Click the question mark for a hint What other organ in the body is prone to hypoperfusion injury?
Here is another patient who had a thrombotic infarct 2 weeks prior to this CT and now presents with new cognitive deficits.
What do you think happened?
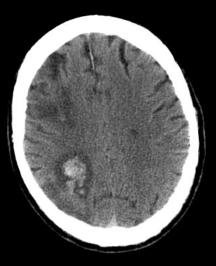
The degree of effacement here is consistent with an infarct that occurred at least a few days prior.

